
At A Glance
- Biologic eye drops, which have been used in ophthalmic practices for almost half a century, are often reserved for patients who have not responded to all other treatments or those who have severe recalcitrant ocular surface disease.
- Platelet-rich plasma is a perfect substitute lubricant for the ocular surface because it not only mirrors the pH and osmolarity of our natural tears, but also incorporates various healing growth factors that can mediate corneal tissue repair.
- Because their safety and efficacy is comparable to that of traditional therapies, biologics should not be used only as a last resort.
Biologic, or blood-derived, eye drops have been used in ophthalmic practices to treat many severe ocular surface conditions for almost half a century. They are often reserved for patients who have not responded to all other treatments or those who have severe recalcitrant ocular surface disease (OSD), but they don’t have to be a last resort. Instead of waiting to reach a specific stage of severity, consider using biologics earlier to preserve the ocular surface and save patients the sequelae.
There is no question that the inflammatory nature of dry eye disease (DED) has a negative effect on patient quality of life. Whether you are exploring blood biologics for the first time, or you have successfully incorporated them into your practice, it’s beneficial to examine the diverse options and understand common applications and scenarios where these drops can be effectively used. (For a brief refresher on biologics, see Biologics, Explained.)
BIOLOGICS, EXPLAINED
Biologics are products made from human blood, specifically platelets. Human platelets, once thought to only play a role in blood coagulation, are now recognized as key players in healing damaged tissue. That’s because platelets contain several growth factors, chemokines, and cytokines that are crucial for wound healing and reducing inflammation.1,2 This newfound understanding has led to widespread use of platelet-derived products in regenerative medicine, addressing issues such as skin rejuvenation and muscle and joint regeneration.1
The use of blood-derived eye drops stems from the fact that many of the growth factors and proteins found in tear film are also present in similar concentrations in platelets and plasma.3 The main platelet-derived products used in eye care are autologous serum (AS) and platelet-rich plasma (PRP). However, other platelet-derived products, such as platelet-rich fibrin (PRF), have also been developed, opening avenues for expanded applications.
PRP
PRP is simply platelets in plasma, after all other blood cells have been removed. To make PRP, unclotted blood is collected from the patient and spun in a centrifuge to separate components.1,2 Red and white blood cells settle at the bottom, while platelets and plasma stay on top and are collected to be used as eye drops (Figure 1). Unlike artificial tears, PRP is a perfect substitute lubricant for the ocular surface, as it not only mirrors the pH and osmolarity of our natural tears, but also incorporates various healing growth factors that can mediate corneal tissue repair.1

Figure 1. PRP is separated via centrifugation. The clear, yellowish layer at the top is PRP. At the bottom is where red blood cells have settled.
AS
AS is considered platelet-poor because platelets are eliminated in the process of its production. To make AS, clotted blood is spun in a centrifuge.1 Clotting of blood causes platelets to release growth factors. Centrifugation separates the blood components, resulting in the activated platelets settling at the bottom alongside red blood cells. The serum left on top is then collected and dispensed as eye drops.
Although AS and PRP may seem similar, there are some notable differences between the two:
- AS does not contain platelets, and therefore has significantly lower growth factor levels when compared with PRP.
- AS contains proinflammatory cytokines derived from leukocyte degradation and high levels of TGF-Β, which may induce negative effects on tissue regeneration.4
- AS is diluted with saline before dispensing to reduce the concentration of inflammatory cytokines.4 Serum dilution leads to an even further decrease in growth factors, potentially limiting its beneficial effects. The most common concentration used in clinical studies for AS is 20%, whereas PRP can be dispensed without any dilution at 100% concentration.
PRF
PRF is a clot-like product that contains the greatest amount of platelets. Thus, it contains more growth factors and can potentially be more effective at healing (Figure 2). Additionally, the growth factors in PRF are released slowly over 7 to 10 days due to its fibrin network, whereas PRP releases growth factors immediately in the absence of a dense fibrin network.5

Figure 2. An example of PRF, a clot-like product rich in platelets.
PRF preparation involves high-speed centrifugation, activating platelets and converting fibrinogen to fibrin, which polymerizes into a 3D clot, trapping platelets and leukocytes.6 This PRF membrane can then serve as a natural scaffold, releasing epitheliotropic factors and promoting cell proliferation and migration.5,6
BUT WAIT, THERE’S MORE (ACRONYMS)
It’s easy to get lost in the various acronyms. You’ll also hear/see PRGF, APL, L-PRP, and I-PRF. These variations are the result of different speeds and times of spin in the centrifuge, yielding a different ratio of cell types.
Plasma rich in growth factors (PRGF), also known as activated PRP, is derived from PRP by adding a coagulant, such as calcium chloride, which activates the platelets to release growth factors before it is dispensed for use.7 It is unclear whether this additional step of activating the platelets produces any further increase in healing, as no studies are available that compare the two methods. The concentration of platelets in PRGF is similar to PRP.
Autologous platelet lysate (APL), also derived from PRP, uses a freeze-thaw-shock method to lyse, or activate, the platelets before dispensing the drops.8
Leukocyte and PRP (L-PRP) is PRP that contains leukocytes and is thought to be helpful in fighting microbes. Injectable PRF (I-PRF) has a more liquid gel consistency. (Neither of these last two are used much in the ophthalmic space, but they are worth noting in the event they do come up.)
Because blood biologics are a promising treatment, continued research will likely expand this list, introducing new products that may have more specific purposes in eye care.
1. You J, Hodge C, Hoque M, Petsoglou C, Sutton G. Human platelets and derived products in treating ocular surface diseases – a systematic review. Clin Ophthalmol. 2020;14:3195-3210.
2. Alio JL, Rodriguez AE, Ferreira-Oliveira R, Wróbel-Dudzińska D, Abdelghany AA. Treatment of dry eye disease with autologous platelet-rich plasma: a prospective, interventional, non-randomized study. Ophthalmol Ther. 2017;6(2):285-293.
3. Soifer M, Tovar A, Wang M, et al. A multicenter report of the use of plasma rich in growth factors (PRGF) for the treatment of patients with ocular surface diseases in North America. Ocul Surf. 2022;25:40-48.
4. Bernabei F, Roda M, Buzzi M, Pellegrini M, Giannaccare G, Versura P. Blood-based treatments for severe dry eye disease: the need of a consensus. J Clin Med. 2019;8(9):1478.
5. Kobayashi E, Flückiger L, Fujioka-Kobayashi M, Sawada K, et al. Comparative release of growth factors from PRP, PRF, and advanced-PRF. Clin Oral Investig. 2016;20(9):2353-2360.
6. Camacho C, Rojas E. Platelet-rich fibrin membrane for pterygium surgery: literature review and feasibility assessment. Cureus. 2021;13(9):e17884.
7. López-Plandolit S, Morales MC, Freire V, Grau AE, Duran JA. Efficacy of plasma rich in growth factors for the treatment of dry eye. Cornea. 2011;30:1312-1317.
8. Fea AM, Aragno V, Testa V, et al. The effect of autologous platelet lysate eye drops: an in vivo confocal microscopy study. Biomed Res Int. 2016;2016:8406832.
WHY USE BIOLOGICS FOR OSD?
Studies have demonstrated the efficacy of autologous serum (AS), platelet-rich plasma (PRP), and plasma rich in growth factors eye drops in the treatment of moderate to severe DED and nonhealing corneal ulcers.1 Alio et al showed that post-LASIK dry eye symptoms improved in 85% of patients treated with PRP (Figure).2
Unlike artificial tears, PRP is a perfect substitute lubricant for the ocular surface, as it not only mirrors the pH and osmolarity of our natural tears, but also incorporates various healing growth factors that can mediate corneal tissue repair.3 PRP eye drops are often administered four to six times daily for 3 months and repeated as needed. PRP eye drops have also been used to manage recurrent corneal erosions. Lee et al found a significantly lower frequency of recurrence in eyes receiving PRP eye drops.4
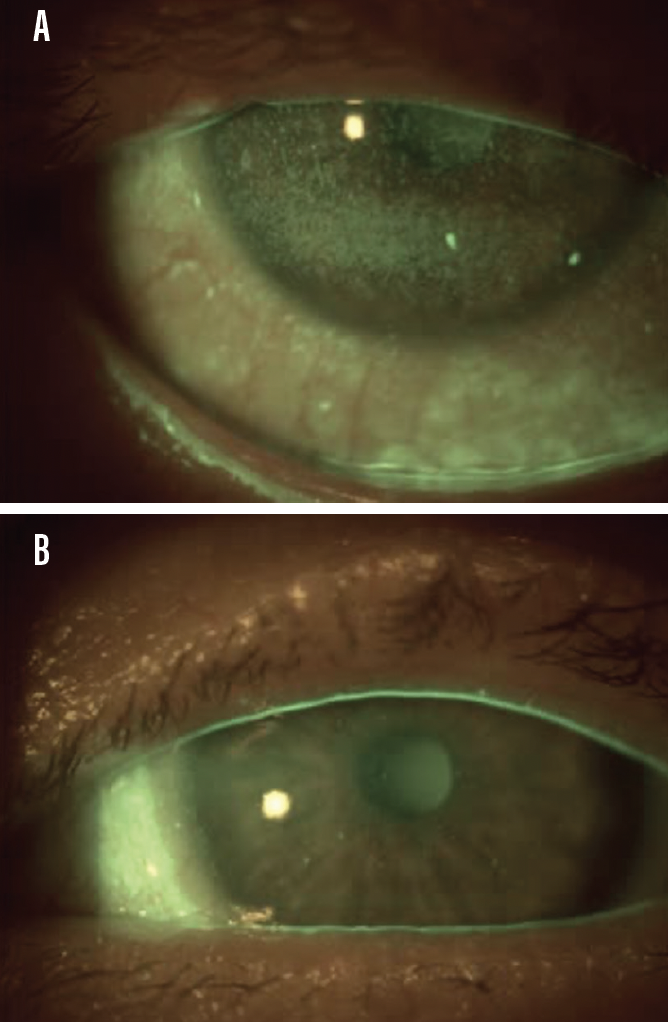
Figure. This patient had persistent epithelial defects secondary to Sjögren syndrome (A), which were resolved with the use of PRP eye drops four times daily for 3 months (B).
Neurotrophic keratopathy (NK) is a rare, but sight-threatening condition caused by a reduction or absence of corneal sensation, and its treatment is often challenging.5 Many recombinant growth factors and cytokines have been used to treat NK and have shown favorable therapeutic responses.6 However, the use of recombinant growth factors is expensive. A more cost-effective approach is the use of a patient’s own blood-derived products to induce tissue regeneration. A study by Sanchez-Avila et al found PRGF eye drops to be a safe and effective therapeutic option for patients with stages 2 to 3 of NK, resulting in high rates of corneal healing.7
Moreover, an in vivo confocal microscopy study demonstrated evidence that platelet-derived eye drops increased corneal subbasal nerve plexus density, suggesting a possible pathway to managing patients with damaged corneal nerves.8 Injection of PRP into the lacrimal gland has also been shown to be a technique in the treatment of severe dry eye, improving tear film parameters through subjective and objective assessment.9
Although more studies are still needed to compare the different blood biologics, PRP has been shown to be superior to AS due to its higher concentration of platelets and platelet-derived growth factors.8,10 A small study by Hwang et al found that AS eye drops might not be effective for the treatment of secondary Sjögren syndrome because of elevated serum proinflammatory cytokine levels.11
Platelet-rich fibrin (PRF) application has been widely described in dentistry, orthopedics, plastic surgery, and otorhinolaryngology.6,12 However, its use in ophthalmology is relatively new, being most commonly used in the management of corneal and ocular surface pathologies.13 A case report by Rahhal et al used PRF membrane to cover a corneal dellen and found positive results.14 PRF has also been used for pterygium repair, and these small studies have concluded that PRF membrane is a safe, effective, and promising method for pterygium surgery with low rates of recurrence and complications.13
IMPLEMENTING BIOLOGICS: WHEN TO START
From the evidence, it is clear that biologic drops can be used to treat many forms of DED.2,3 The drops do not simply act as a “bandage,” but they actually address the root cause of DED (ie, inflammation), and lead to cellular repair and healing. Furthermore, biologic drops can easily be combined with other treatment options, such as intense pulsed light therapy or immunomodulators, to target the multifactorial disease process.
Biologic drops can be used for mild, moderate, or severe dry eye and for patients simply wanting more natural options. Biologics are arguably safer than any medicated eye drops, and once we understand their epitheliotropic function in repairing the ocular surface, it is easy to see why they should not be reserved for only treating end-stage dry eye.
HOW DO WE ACCESS BIOLOGICS?
Access to biologics has been a bit challenging (due to a lack of standardization protocol, different state laws on scope, and limited availability of systems that make blood biologics), but it is improving. Optometrists can implement a system in their own practices or work with local laboratories and pharmacies to establish access to autologous drops.
Additional Reading

For more on platelet-rich plasma eye drops, read my article on five common myths related to the use of PRP in the treatment of patients with dry eye.
In addition to accessibility, the economic cost and financial sustainability can also be a barrier to this treatment. Biologic drops are generally not covered by insurances, and prices can range from $400 to $600 for a 3-month supply. However, once patients are educated about the potential benefits of PRP therapy, they are often willing to try it. Additionally, there are foundations that help patients access their medications.
With more than 50% of patients experiencing some level of dry eye, incorporating biologics in your clinic can be a powerful tool.
- 1. Sanchez-Avila RM, Merayo-Lloves J, Riestra AC, et al. The effect of immunologically safe plasma rich in growth factor eye drops in patients with Sjögren syndrome. J Ocul Pharmacol Ther. 2017;33(5):391-399.
- 2. Alio JL, Pastor S, Ruiz-Colecha J, Rodriguez A, Artola A. Treatment of ocular surface syndrome after LASIK with autologous platelet-rich plasma. J Refract Surg. 2007;23(6):617-619.
- 3. You J, Hodge C, Hoque M, Petsoglou C, Sutton G. Human platelets and derived products in treating ocular surface diseases – a systematic review. Clin Ophthalmol. 2020;14:3195-3210.
- 4. Lee JH, Kim MJ, Ha SW, Kim HK. Autologous platelet-rich plasma eye drops in the treatment of recurrent corneal erosions. Korean J Ophthalmol. 2016;30(2):101-107.
- 5. Sacchetti M, Lambiase A. Diagnosis and management of neurotrophic keratitis. Clin Ophthalmol. 2014;8:571-579.
- 6. Anitua E, de la Fuente M, Muruzabal F, Riestra A, Merayo-Lloves J, Orive G. Plasma rich in growth factors (PRGF) eye drops stimulates scarless regeneration compared to autologous serum in the ocular surface stromal fibroblasts. Exp Eye Res. 2015;135:118-126.
- 7. Sanchez-Avila RM, Merayo-Lloves J, Riestra AC, et al. Treatment of patients with neurotrophic keratitis stages 2 and 3 with plasma rich in growth factors (PRGF-Endoret) eye-drops. Int Ophthalmol. 2018;38(3):1193-1204.
- 8. Fea AM, Aragno V, Testa V, et al. The effect of autologous platelet lysate eye drops: an in vivo confocal microscopy study. Biomed Res Int. 2016;2016:8406832.
- 9. Mohammed MA, Allam IY, Shaheen MS, Lazreg S, Doheim MF. Lacrimal gland injection of platelet rich plasma for treatment of severe dry eye: a comparative clinical study. BMC Ophthalmol. 2022;22(1):343.
- 10. Anitua E, Muruzabal F, de la Fuente M, Riestra A, Merayo-Lloves J, Orive G. PRGF exerts more potent proliferative and anti-inflammatory effects than autologous serum on a cell culture inflammatory model. Exp Eye Res. 2016;151:115-121.
- 11. Hwang J, Chung SH, Jeon S, et al. Comparison of clinical efficacies of autologous serum eye drops in patients with primary and secondary Sjogren syndrome. Cornea. 2014;33(7):663-667.
- 12. Grecu AF, Reclaru L, Ardelean LC, Nica O, Ciuca EM, Ciurea ME. Platelet-rich fibrin and its emerging therapeutic benefits for musculoskeletal injury treatment. Medicina (Kaunas). 2019;55(5):141.
- 13. Camacho C, Rojas E. Platelet-rich fibrin membrane for pterygium surgery: literature review and feasibility assessment. Cureus. 2021;13(9):e17884.
- 14. Rahhal-Ortuño M, Fernández-Santodomingo AS, Martínez-Rubio C, Barranco-González H, Almor-Palacios I, Rodrigo-Hernández A. Use of plasma rich in growth factors (PRGF-Endoret®) fibrin membrane to cover corneal dellen. Rom J Ophthalmol. 2021;65(3):293-295.