
The role of eyelid malposition in ocular surface disease and how to address it.
At A Glance
- Eyelid malposition occurs when the eyelid shifts to an abnormal anatomic position.
- Of symptomatic patients with dry eye, 60% have compromised lid closure due to eyelid malposition.
- Regardless of the type of eyelid malposition, hallmark symptoms may present similarly as foreign body sensation, excessive tearing, redness, and ocular irritation. There are differences in signs and symptoms.
- Although symptoms play an important role in identifying eyelid malposition, a careful objective examination of the eyelids is critical in determining the malposition and recommending the appropriate treatment.
In recent years, the role that the eyelids play in dry eye disease (DED) has drawn increasing attention. Addressing lid disease is critical in managing inflammation and reducing the perpetual cycle of DED. Eyelids also play a key role in the complex tear dynamics needed to maintain a stable tear film, prevent ocular surface desiccation, and preserve healthy tear mechanics with each blink.1
An eyelid malposition, as the name suggests, occurs when the eyelid shifts to an abnormal anatomic position. Blackie et al found that more than 60% of symptomatic patients with dry eye had compromised lid closure due to eyelid malposition.2,3 Conversely, 80% of asymptomatic patients had healthy functioning eyelids that demonstrated good lid seal.2
If you are treating a patient’s ocular surface but not addressing the role that eyelids play in their function to protect the eye, you are fighting an uphill battle by treating the inflammation without treating its cause. For this reason, managing eyelid malposition is imperative in successfully treating DED.
SIGNS AND SYMPTOMS OF EYELID MALPOSITION
Regardless of the type of eyelid malposition, the hallmark symptoms may present similarly as foreign body sensation, excessive tearing, redness, and ocular irritation. However, there are differences in signs and symptoms that are important to note. For example:
- Patients with ectropion often present with inferior corneal or conjunctival staining and keratinization of the palpebral conjunctiva due to exposure and chronic inflammation.
- Patients with entropion report foreign body sensation or pain, especially when reading or looking down; mucus discharge; and crusting around the eyelids and inferior keratoconjunctivitis.
- In floppy eyelid syndrome, one may see periodic episodes of papillary conjunctivitis and hyperemia, especially upon awakening.
Although symptoms play an important role in identifying eyelid malposition, a careful objective examination of the eyelids is critical in determining the malposition and recommending the appropriate treatment. Below are some important tests to consider.
Lower Eyelid Position
Begin the external examination by looking at the position of the lower eyelids for any evidence of ectropion, entropion, or scleral show. Mild ectropion can be seen as a subtle eversion of the lower eyelid margin outwards. Moderate ectropion involves a step-off of the eyelid from the globe and severe ectropion can be seen as frank eversion of the tarsus eyelid (Figure 1).
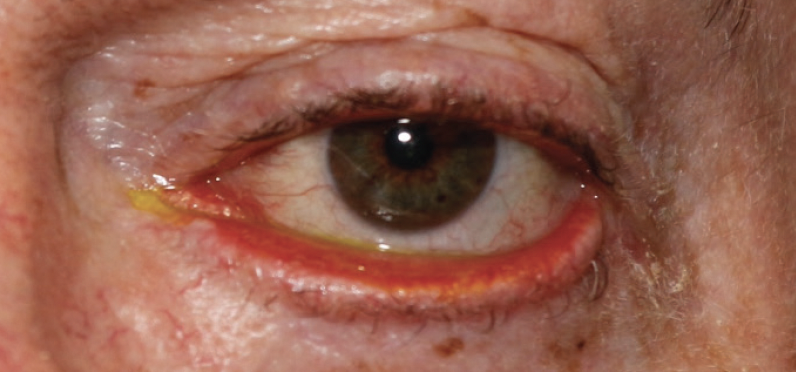
Figure 1. Ectropion with keratinization of the palpebral conjunctiva.
Photo courtesy of Helen K. Lee, OD.
Entropions cause the lower eyelids to roll inwards. If entropion is not seen but is suspected, one may induce entropion by having the patient forcefully squeeze their eye closed while the clinician holds the upper eyelid open.
Eyelid Retraction Evaluation
Next, with the patient’s head perpendicular to the floor, measure the lower or upper eyelid margin relative to the inferior or superior limbus in millimeters, respectively. When the eyelids are retracted, the upper eyelids may not meet the lower eyelids, resulting in lagophthalmos (Figure 2). Any amount of scleral show can predispose patients to DED. Patients with prominent globes are particularly at risk for age-related eyelid retraction, as this creates an anatomic disadvantage, allowing gravity to pull the lower eyelid down further, like a belt that falls below a big belly.
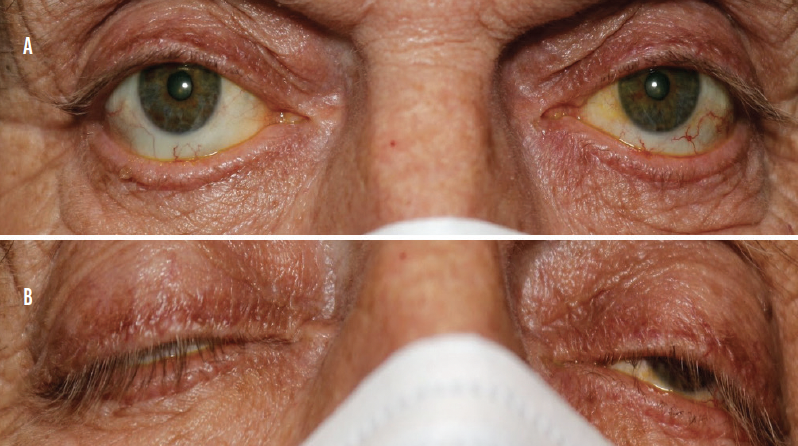
Figure 2. Patient with significant bilateral lower eyelid retraction with inferior scleral show (A) and lagophthalmos OU (B; OS > OD).
Photo courtesy of Helen K. Lee, OD.
Lid Laxity Evaluation
Another important test is to consider is to check for lid laxity or tone of the lower eyelids by performing the “eyelid snap back test,” where the lower eyelid is pulled inferiorly away from the globe and then allowed to return to position (Figure 3).4 In case of poor lid laxity, the lid will not return quickly to its normal anatomic position and may require a blink to regain the normal position. Eyelid laxity can lead to eyelid closure issues, including incomplete blink and lagophthalmos.

Figure 3. Shows patient with lower eyelid laxity.
Photo courtesy of Mahnia Madan, OD, FAAO.
Lagophthalmos Evaluation
Checking for lagophthalmos should be part of every dry eye evaluation. Have the patient lean their head back in the exam chair and close their eyes gently while you shine a transilluminator where the lid margins meet. Any amount of opening should be noted as lagophthalmos in millimeters (Figure 4).

Figure 4. This patient with lagophthalmos has an opening about 1 mm to 2 mm between his palpebral fissure.
Photo courtesy of Marcus J. Ko, MD, of Nevada Eye Plastic Surgery.
Alternatively, a clinician can perform the Korb-Blackie lid light test (Figure 5) by darkening the room and placing the transilluminator on the closed upper eyelid and watching for any light escaping from the palpebral fissure. Light escaping indicates incomplete or inadequate lid seal. The amount of visible light can be quantified on a scale of zero to three (0 = no light, 1 = minimal light, 2 = moderate light, and 3 = severe light).

Figure 5. Patient with mild lagophthalmos as seen using the Korb-Blackie lid light test.
Photo courtesy of Mahnia Madan, OD, FAAO.
Floppy Eyelid Evaluation
Before placing the patient behind the slit lamp, pull the upper eyelid up and out temporally to see how far the eyelid can be displaced. Floppy eyelid syndrome (Figure 6) is an underdiagnosed eyelid malposition that presents with hyperlaxity of the upper and lower eyelids.4 These eyelids tend to evert easily, putting the cornea and conjunctiva at risk for making direct contact with the patient’s pillow while sleeping, especially if they tend to sleep on their stomach or sides. Floppy eyelid syndrome can be associated with ocular and systemic diseases, notably keratoconus and obstructive sleep apnea.5

Figure 6. Patient with severe floppy eyelid syndrome.
Photo courtesy of Marcus J. Ko, MD, of Nevada Eye Plastic Surgery.
CAUSES OF EYELID MALPOSITION
Most eyelid malposition is caused by involutional changes, where the structures of the eyelid becomes loose or lax with aging, resulting in medial displacement of the lateral canthus and loosening of the eyelid anchoring mechanism. Proper canthal anchoring pulls the eyelids tight and is critical in producing a forceful blink, which in turn acts to facilitate the pumping mechanism that washes tears across the eye and down the canaliculus.6 With these involutional changes, one may see signs of incomplete blink or lagophthalmos and symptoms of significant tearing, in addition to DED. Eyelid malposition can also be due to paralytic causes, such as Bell palsy or trauma to the facial nerve. Weakness or paralysis of the facial nerve results in poor orbicularis function and the inability to close the eyelid (Figure 7).

Figure 7. Patient with paralytic poor lid closure.
Photo courtesy of Helen K. Lee, OD.
Cosmetic surgeries such as upper and lower blepharoplasty or ptosis repair can also cause eyelid malposition. Too much skin removed from the upper or lower eyelids during surgery or ptosis overcorrection can lead to lagophthalmos. Additionally, the orbicularis muscle can be damaged or weakened by surgery and lead to poor eyelid closure.
Lastly, eyelid retraction can be seen in thyroid eye disease, where inflammation and scarring of the periorbital tissues can cause proptosis and/or eyelid retraction, again leading to weakened lid closure and lagophthalmos.
Careful history and evaluation of the eyelids are critical in determining the cause and type of malposition and recommending the appropriate treatment.
NONSURGICAL MANAGEMENT OF EYELID MALPOSITION
Not all eyelid malposition requires surgical treatment, and optometrists play a critical role in managing these patients by optimizing their DED. Remember that eyelid malposition is often only one of the factors contributing to DED. A thorough case history, along with a comprehensive anterior segment examination, is imperative in identifying other factors. Managing as many of the contributing factors as possible in a tailored and systematic approach will help bring much needed relief to your patients.
If the eyelid malposition is relatively mild, consider starting off by having the patient use artificial tears during the day, along with eye ointments at night to help provide additional moisture while sleeping. Intensive moisturization of the eyelid skin and face can help minimize mild ectropion and lagophthalmos if the patient has dry, tight periocular skin. This can be achieved by applying a high-quality moisturizer or bland eye ointment to the lower eyelid skin and cheeks at least twice daily. Noninvasive in-office treatments with radio frequency can also be helpful in patients with mild lid laxity to improve eyelid apposition. Radio frequency uses high frequency electrical currents to stimulate fibroblasts and collagen production, which results in skin tightening. Often, patients will require one treatment for every decade of life to see results. If the patient has frank entropion, tautly taping the lower eyelid down to their cheek can give them some temporary relief until surgery.
Moisture chamber goggles, such as eyeseals 4.0 hydrating sleep mask (Eye Eco), or taping the eyelids closed can prevent unintended exposure while sleeping. Patients with mild to moderate floppy eyelids should also be instructed to avoid sleeping on their sides or stomach to minimize the risk of their ocular surface making contact with their pillow. For these patients, the clinician should also consider a referral to their primary care doctor for sleep apnea evaluation, especially if they have symptoms of sleep apnea. These patients may snore loudly, be chronically tired during the day, wake up gasping for air, or their partner may state that they stop breathing during sleep.
If patients have upper eyelid paralysis and there is potential for improvement in function, external lid weights (eg, Blinkeze External Lid Weights [MedDev Corporation]) can be used to help eyelid closure. These adhesive lid weights use gravity to weigh down the upper eyelid and create a more natural, complete blink and closure (Figure 8).
![<p>Figure 8. A patient with paralytic lagophthalmos (A) has a trial weight taped on the eyelid to provide complete closure (B). Depending on the patient’s prognosis, the optometrist may either order a temporary eyelid weight (eg, Blinkeze External Lid Weights [MedDev Corporation]) and adjust the weight as the patient improves, or the patient may be referred to an oculoplastic surgeon for surgical gold weight placement.<br /> Photo courtesy of Helen K. Lee, OD</p>](https://core4-cms.imgix.net/issue-2367/0323_F5_Fig8.png)
Figure 8. A patient with paralytic lagophthalmos (A) has a trial weight taped on the eyelid to provide complete closure (B). Depending on the patient’s prognosis, the optometrist may either order a temporary eyelid weight (eg, Blinkeze External Lid Weights [MedDev Corporation]) and adjust the weight as the patient improves, or the patient may be referred to an oculoplastic surgeon for surgical gold weight placement.
Photo courtesy of Helen K. Lee, OD
Punctal plugs can be a key player in patients with lagophthalmos by increasing tear volume and helping to reduce dependency on artificial tears while preserving the patient’s natural tear film. Read more about this option in the article “Put a Plug in Dry Eye” by Rebecca Miller, OD.
Patients should also be carefully examined for blepharitis and meibomian gland dysfunction (MGD). The presence of MGD leads to poor quality and quantity of meibum production, causing tear film instability. Literature suggests that as many as 86% of patients with dry eye have MGD6 and that more than 58% of patients have Demodex blepharitis.7
At-home lid hygiene, in combination with in-office treatments with microblepharoexfoliation, thermal pulsation, or intense pulsed light therapy, should be used to help manage these conditions. Intense pulsed light therapy, combined with meibomian gland expression, has been found to treat MGD safely and effectively and improve meibomian gland structure and function over time.8,9
In addition, one may consider the use of immunomodulators to help manage ocular surface inflammation. If there is significant corneal staining or nonresolving epithelial defects, we can also turn to autologous serum and platelet rich plasma to help heal the corneal surface.10
Another major cause of dry eye is the use of systemic medications such as oral contraceptives, antidepressants, antihistamines, and antihypertensives. Although we may not be able to modify a patient’s drug therapies, we can manage expectations and guide our DED treatment plan accordingly.
If a patient’s eyelid condition is relatively mild and their DED has been optimized with nonsurgical treatment, but they still have notable symptoms, a referral to oculoplastics would be appropriate. In cases where the patient has ectropion or any degree of entropion, earlier surgical intervention is recommended to avoid having to undergo more extensive surgery. Just as you would manage DED prior to sending the patient for refractive consult, the same is true in this case.
SURGICAL MANAGEMENT OF EYELID MALPOSITION
Although surgical techniques vary between surgeons, some common surgical treatments are outlined below.
Ectropion and entropion often require horizontal eyelid tightening to eliminate laxity, as this is the primary cause of the eyelid malposition. In the case of severe ectropion, where there is a shortage of skin, a full thickness skin graft may need to be placed in the lower eyelid.6
Lower eyelid retraction repair may involve placement of a spacer graft directly into the lower eyelid to help build up or scaffold the lower eyelid upwards into a more normal position.
In instances where a permanent facial palsy prevents the patient from blinking or completely closing the eye and there is no potential for improvement, a gold or platinum weight may be surgically implanted into the upper eyelid to augment the effect of gravity and help the upper eyelid close. In cases of severe exposure keratopathy or a neurotrophic cornea, a temporary or permanent tarsorrhaphy may be placed to surgically fuse the upper and lower eyelids together, giving the cornea a chance to heal.6
Floppy eyelid repair often requires excising a wedge of redundant or excess eyelid tissue and then suturing the two edges together, effectively tightening the eyelid and creating improved apposition of the lid to the globe.6
When lagophthalmos and eyelid retraction is caused by thyroid eye disease, treatments using oral or intravenous steroids or teprotumumab-trbw (Tepezza, Horizon Therapeutics) infusions may be helpful. In severe cases of exposure due to proptosis, an orbital decompression may be required. Decompression fractures the bones of the orbit in a controlled manner to expand the orbital volume, allowing the globe to fall back into the orbit and reducing the proptosis and exposure of the eye.
THE MAKINGS OF A WINNING DRY EYE TREATMENT PROTOCOL
It is essential that the clinician recognize any eyelid malposition and its contribution to dry eye and ocular symptoms and signs. Thus, assessment of eyelid position should be part of every dry eye consultation. Additionally, partnering with an oculoplastic surgeon to treat eyelid conditions is critical to the success of any comprehensive dry eye treatment plan.
- 1. Chhadva P, McClellan AL, Alabiad CR, Feuer WJ, Batawi H, Galor A. Impact of eyelid laxity on symptoms and signs of dry eye disease. Cornea. 2016;35(4):531-535.
- 2. Korb D, Blackie C, Nau A. Prevalence of compromised lid seal in symptomatic refractory dry eye patients and asymptomatic patients. Invest Ophthalmol Vis Sci. 2017;58:2696
- 3. Korb DR, Blackie CA. Treating inadequate lid seal in patients with dry eye using an overnight ointment reduces discomfort upon awakening and overall dry eye symptoms. Invest Ophthalmol Vis Sci. 2016;57(12):6189.
- 4. Holds J, Chang W, Daily R, et al. Section 7: orbit, eyelids, and lacrimal system 2017-2018 basic and clinical science course. American Academy of Ophthalmology.
- 5. Salinas R, Puig M, Fry CL, Johnson DA, Kheirkhah A. Floppy eyelid syndrome: a comprehensive review. Ocul Surf. 2020;18(1):31-39.
- 6. Shriver EM, Erickson BP, Kossler AL, Tse DT. Ophthalmic Plast Reconstr Surg. 2016;32(5):378-385.
- 7. Lemp MA, Crews LA, Bron AJ, Foulks GN, Sullivan BD. Distribution of aqueous-deficient and evaporative dry eye in a clinic-based patient cohort: a retrospective study. Cornea. 2012;31(5): 472-478.
- 8. Trattler W, Karpecki P, Rapoport Y, et al. The prevalence of Demodex blepharitis in US eye care clinic patients as determined by collarettes: a pathognomonic sign. Clin Ophthalmol. 2022;16:1153-1164.
- 9. Rong B, Tang Y, Tu P, et al. Intense pulsed light applied directly on eyelids combined with meibomian gland expression to treat meibomian gland dysfunction. Photomed Laser Surg. 2018;366):326-332.
- 10. Kassir R, Kolluru A, Kassir M. Intense pulsed light for the treatment of rosacea and telangiectasias. J Cosmet Laser Ther. 2011;13(5):216-222.